What happens to the x-ray when they pass through the patient?
There are five possible ways for the x-ray photon to interact with the matter of the patient (and they may do more than one type).
- Coherent Scatter - the photon hits the object and changes direction with no absorbtion of energy. This type of interact is detrimental to diagnostic radiography as they can strike the film and degrade image quality, or strike the radiographer exposing them to radiation
- Photoelectric Effect - the photon hits the patient ans is totally absorbed, and ejects and electron from an inner shell of a tissue atom, the space is then filled by another electron which causes a characteristic x-ray to be given off. The probability of this reaction occuring is in direct proportion to a tissues atomic number. It is this atomic number dependence on the photoelectric effect that creates the contrasts seen between the different opacities on an image.
- Compton Scattering - photon interacts with a peripheral shell electron, the electron is ejected and the phot is scattered at different angles. This is disadvantagous as it degrades the image and causes personell exposure.
- Pair production - no relevance to x-ray production
- Photodisintegration - no relevance to x-ray production
That's enough learning for today, I have other plans. This afternoon I am going to a BBQ with some friends of mine. Should be good, but no drinking because I have to drive (stupid zero limit!) We are suppose to bring our own meat but I don't know what I should bring? Its very hot so as long as I don't have to cook any thing is good I guess. Wish Ducky had a pool though.
Listening to The Killers "Sam's Town" but on the road I am thinking that Rocky Horror Picture Show or Pricilla Queen of the Desert Soundtracks might be the go. Feel like vamping!!

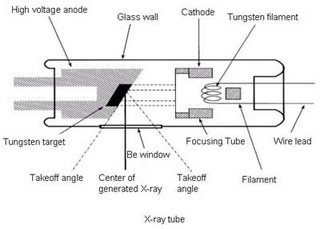 X-rays are electromagnetic radiation produced by electron interactions outside the nucleus. In order to produce this interaction an x-ray tube is used. The tube is made of glass and contains within it a wire filament cathode, and a tungsten anode (which may be stationary or rotating). An electric current is passed through the cathode filament causing it to heat up and release electrons into an electron cloud around the filament. The higher the mA, the greater the current passing through the filament, and therefore the more electrons in the cloud. The electron cloud remains stationary unless a voltage differential (kVp) exists between the cathode and the anode. Since electrons are negatively charged the positively charged anode attracts the electrons to it. The greater the potential difference (kVp) between the cathode and anode, the faster the velocity of the electrons. This means that the electrons strike the anode with greater energy and so the x-rays produced have higher energy. The greater the energy of an x-ray the greater its penetration of matter.
X-rays are electromagnetic radiation produced by electron interactions outside the nucleus. In order to produce this interaction an x-ray tube is used. The tube is made of glass and contains within it a wire filament cathode, and a tungsten anode (which may be stationary or rotating). An electric current is passed through the cathode filament causing it to heat up and release electrons into an electron cloud around the filament. The higher the mA, the greater the current passing through the filament, and therefore the more electrons in the cloud. The electron cloud remains stationary unless a voltage differential (kVp) exists between the cathode and the anode. Since electrons are negatively charged the positively charged anode attracts the electrons to it. The greater the potential difference (kVp) between the cathode and anode, the faster the velocity of the electrons. This means that the electrons strike the anode with greater energy and so the x-rays produced have higher energy. The greater the energy of an x-ray the greater its penetration of matter. 


{kind=link}